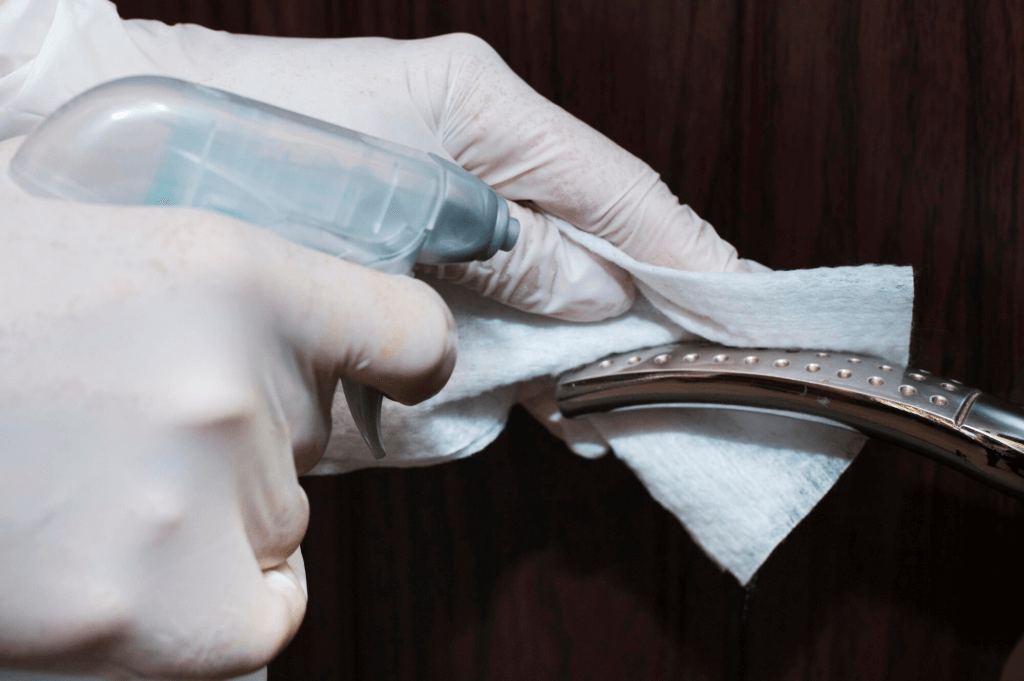
2. Match the Disinfectant to the Equipment
This is where people get it wrong. A surface-grade spray won’t cut it for semi-critical items. And alcohol wipes can damage sensitive equipment if used incorrectly.
There are three classes of items to consider:
- Non-critical (contact with intact skin): blood pressure cuffs, bed rails
- Semi-critical (contact with mucous membranes): thermometers, ultrasound probes
- Critical (penetrate tissue or bloodstream): surgical tools, scopes
Use hospital-grade disinfectants that are:
- TGA-approved
- Non-corrosive
- Fast-drying
- Suited to the device material (check manufacturer guidelines)
And yes, that means using different products for different items. Convenience shouldn’t override compatibility.
6. Document Everything
You don’t need a full ISO system. But you do need proof of process. Especially in health environments where regulators, insurers, and patients expect transparency.
At minimum:
- Keep daily logs of disinfected equipment
- Note who did it, when, and what product was used
- Use QR or barcode systems for high-use items if volume justifies it
Cleaning is often invisible work. Documentation makes it accountable.